Foaling Mares and Assistance:
“Parturition is a unique physiologic process that terminates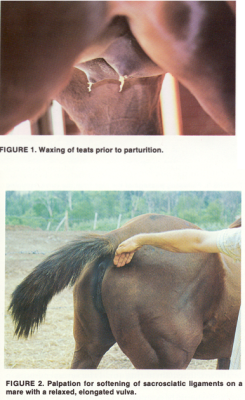 pregnancy and begins the extra-uterine existence of the foal.”
pregnancy and begins the extra-uterine existence of the foal.”
Survival of the foal is dependent on terminal developmental events in utero.  The foal is active and regular fetal motion is necessary for normal musculoskeletal development.  It prepares the fetus to attain actively the correct posture and position during labor.  We expect to see a lot of normal foal activity during the last weeks of a pregnancy.
Signs of imminent parturition normally include udder development with distention of the teats with colostrum, waxing in the final 24 hours, relaxing of the sacro-sciatic ligaments and vulva and softening of the cervix.  Waxing is an important development that is very helpful.  However, some mares wax for days and some never do develop this crystallized secretion. These are more difficult to predict.  Some mares begin to drip their colostrum and sometimes this requires that we collect and save the colostrum. By doing so we will have it when the mare does foal.  Otherwise we would need to use colostrum that has been banked.
Be aware that the mare has four mammary glands but only two teats.  When milking a mare it is usually obvious that there are two streams when the teat is expressed.
Other changes that are noted at the end include relaxing of the sacro-sciatic ligament with obvious sinking of the tail head and the typical “bowl of jelly” wiggle.  This occurs as the result of the hormone relaxin.  The elongation, relaxation, and swelling of the vulva are subtle in the mare.  These changes may not become obvious until a few hours before the birth.
Labor is divided into three stages:
It is difficult to say exactly when stage I begins.  The development of muscle contractions signal the beginning, but this is not readily apparent in every case.  You may see patchy sweating behind the elbows, in the flanks and along the neck as early as 4 hours before the birth.  The mare may be restless and pace in the stall.  She may switch her tail as a sign of discomfort and she may begin to pass progressively smaller piles of loose feces.
Often a mare will get up and down and stretch as if she needs to urinate.  In general she will look agitated and show signs of colic such as looking at her flanks.
The uterine contractions stimulate the foal to move into the normal foaling position with the front legs and head extended.  The cervix dilates in response to the uterine contractions and vaginal passage of the chorioallantoic fluid when the membrane ruptures in the area of the cervical star.  The chorioallantois ruptures when the hooves pass through the cervix.  This is when her “water breaks”.  This marks the end of stage I labor and the beginning of stage II.
Note: if a mare is disturbed in stage I and before the membrane ruptures, she can stop or delay the onset of stage II for hours or even days.
In rare cases the chorioallantois doesn’t rupture as it should and passes with the foal.  When the red, velvet like chorioallantoic membrane appears passing through the lips of the vulva, you are witnessing a red-bag delivery and this is the first of two emergencies that you must be prepared to handle.  This is the placenta and the foal is no longer receiving oxygen from the mare.  It is an emergency and the night nurse attendant must immediately tear or cut the membrane and apply traction to assist in delivering the foal quickly.  If caught early, this foaling complication can be resolved easily.  Normally you should contact the Dr. on call and/or the tech on call.  If they don’t answer, there isn’t time for waiting or even paging a doctor as a couple of minutes can seal the foal’s fate.   You must be ready to manage this complication!
Stage II begins when the mares water breaks  and the brown discolored water breaks.  This water is in fact the waste that the foal has produced during the many months of the pregnancy.  The fetus enters the birth canal and it stretches the soft tissues of the pelvic cavity.  With the appearance of the blue-white glistening amniotic membrane at the vulva, the mare will usually lie down in lateral recumbancy.  Forceful contractions begin with groups of 3 or 4 followed by rest periods of 2-3 minutes.  Most mares will get up and change positions in stage II labor.  It is thought that this is an attempt by the mare to help re-position the foal in the normal presentation.  We normally see one hoof followed very quickly by the other front hoof.  The key thing to consider at this point is which direction the soles of the hooves are pointing.  They should be pointed at the mare’s hocks.  The most forceful contractions occur as the head and shoulders pass through the pelvis.  When the hips clear the vagina, the straining stops and stage II is over.  Stage II can be as short as ten minutes, but is more often around 20 minutes in length.  On rare occasions it can last longer, but if it is delayed, you should be checking to insure that the legs are positioned normally and the head is close behind.  After the chest is delivered the foal will usually rest quietly for a few minutes while the hind legs are still inside the mare.  If the foal hasn’t torn the amnion away from the head at this point, the attendant should step in and remove it.  If you palpate the umbilical cord at this point, you will feel it throbbing as the fetal blood is pumped out of the placenta and into the foal.  The placenta will break about one inch from the abdomen when the mare gets up or when the foal struggles to get up.  The cord should be immediately treated with iodine, taking care not to get it all over the foal.  There have been mares that refuse to lie down and have in fact delivered their foals while standing.  If this happens when you are on duty, you may need to catch the foal.
Stage III involves passage of the fetal membranes.  Although the active straining stops, the uterine contractions continue.  Once the fetal blood vessels are ruptured, the villi collapse and disconnect from the maternal crypts.  The placenta is usually delivered with the allantoic surface outermost.  The mare may show similar signs of discomfort as before the birth.  We may have you administer Banamine or we may just distract the mare by walking her.  These symptoms are usually short lived.  We expect the placenta to pass within 3 hours of the birth.  If the placenta is still in the mare after 3 hours, it is considered a retained placenta.  This means the mare will be treated or lavaged after the
placenta is removed.  Stage III is over when the placenta is passed and the parturition is complete.
Assisting mares in their delivery is often necessary in the hospital environment.  We usually hold pressure on the foals as they are being delivered.  This is known as traction.  We help the foal keep from slipping back into the mare when she rests between contractions and abdominal thrusts.  Frequent checks of the foal’s position are not necessary once you have established the position is correct.  If the presentation is not correct, we describe this abnormal delivery as a dystocia
Our goal when dealing with a dystocia is to save the mare and the foal.  The treatment approach to any dystocia is selected from a list of four different obstetrical methods: reposition, traction, fetotomy or cesarean section.  We select the method and develop a plan that places the highest priority on the mare, next the foal and the economic best interests of the clients.  Every dystocia is an emergency and you must be prepared.  There should be an oxygen tank handy as well as the crash cart for drug support and the monitoring equipment.
Simple dystocias may be an elbow that is flexed at the pelvic brim.  This only requires traction to straighten the leg.  A head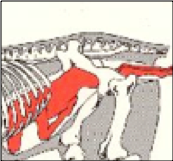 back can be corrected if caught early.  The second foaling emergency that will require quick action is the breech presentation.  As seen in the adjacent photo, this presentation is often delayed and can result in brain damage from oxygen deprivation and or death.  As listed above with a red-bag delivery, contact the doctor and/or tech on call immediately.  If they don’t answer, you can leave a message and then you must act.  Apply simple traction to hasten the delivery and then treat as a normal foal.
back can be corrected if caught early.  The second foaling emergency that will require quick action is the breech presentation.  As seen in the adjacent photo, this presentation is often delayed and can result in brain damage from oxygen deprivation and or death.  As listed above with a red-bag delivery, contact the doctor and/or tech on call immediately.  If they don’t answer, you can leave a message and then you must act.  Apply simple traction to hasten the delivery and then treat as a normal foal.
Most other dystocias will be anesthetized and lifted on the hoist to elevate the hand quarters.  This allows the foal to fall back in the mare and give the veterinarian room to reposition the foal.
Lactation:  The placenta of the mare prevents transfer of maternal antibodies to the fetus in-utero.  The foal depends entirely on passive transfer of the antibodies in the mare’s first milk which is called colostrum.  The absorbtion of the antiboidies in the intestine is very quick in the beginning.  After about 8 hours the intestinal lining changes and the antibodies can no longer get into the blood stream.  This will result in a low IgG test and may necessetate a transfusion of plasma.  However, bacteria can also travel through these “intestinal holes and gain access to the foal’s blood stream.  We can greatly reduce the chances of this by milking the mare as soon as she gets up and squirting this colostrum into the foal’s mouth.  This simple procedure can buy time until they learn how and where to nurse.  The antibodies will have a head start on the bacteria.
An enema may be needed to assist the foal in passing the first manure or bowl movement.  This material is dark green to black and is called meconium.  The enema should be warmed.  If no commercially prepared enema is handy, a 60 cc syringe with 1-2 drops of dish soap shaken can be used and is very productive and inexpensive.  The mare needs to be dewormed with Ivermectin on this birth-day and she may need oxytocin to assist with delivery of the afterbirth.
In regards to the stall: if the stall is bedded in straw, it can be cleaned and replaced with shavings.  We simply want them to foal on straw.  Once parturition is complete, we no longer need the straw.  All wet spots and fecal material should be removed so the foal has good traction when it comes time to get up.
If the mare is still hanging onto the placenta, it can be put in an OB sleeve and the entire mass tied tightly with baling twine.  This keeps the mare from stepping on the placenta and damaging the uterus when it is ripped out.